
This week there has been a slight tweek in my role. I’ve been doing a lot more injections since they have been trying to train up one of my colleagues to do more imaging. There are a lot of steps involved with each administration. Too many in my opinion but that is just that. There are good reasons for performing the tasks as they are performed. I’m going to describe a generic administration for posterity.
Each procedure has its own particular set of preparations that are needed to be adhered to. Some procedures have none as the normal physiology has no effect on the diagnostic outcome. Most patients get dealt with as they come in in order of their arrival except when the procedure requires expedited attention.
The first thing that gets checked is the name and the type of procedure followed by a check of authorization by the consultant in the department. Everything is digitized so a lot of time is spent looking at a screen navigating through the program that is installed on all the computers in the department. Each part of the procedure has its own scheduled time allocated in the diary. It roughly corresponds to the time when we expect the scan to take place. It doesn’t always work out that way but we try.
Each dose is drawn individually and must be checked by another colleague who is authorized to perform this task. This department has a range of banded employees who can only perform certain tasks according to the amount of training that they have. This banding corresponds to the amount of money that they get paid at the end of each month.

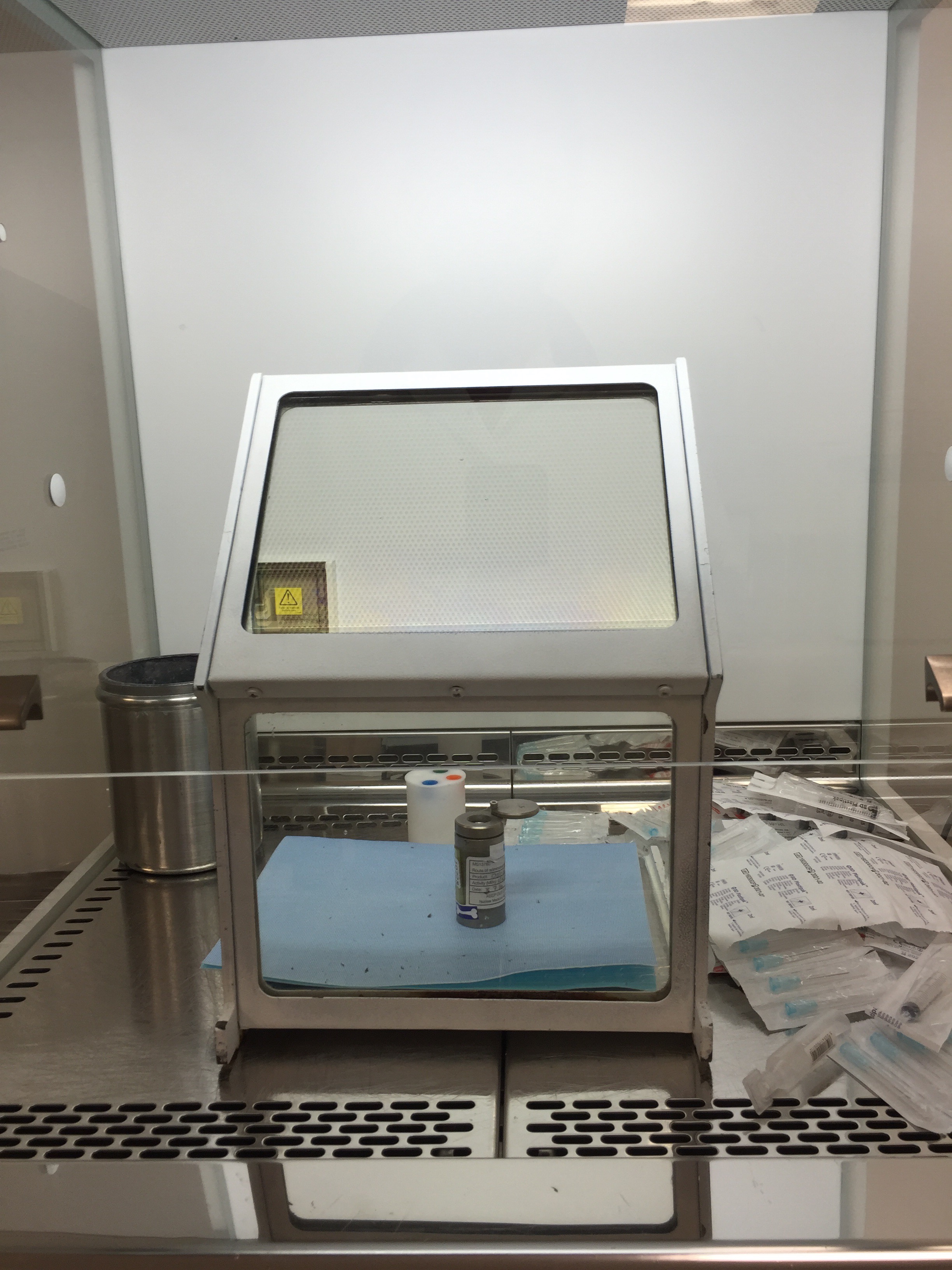
The dose is drawn once the check for authorization takes place. One dose is drawn at a time to prevent the wrong dose being drawn and subsequently administered. The doses are drawn in a fume hood to minimize the chance of environmental contamination being introduced into the dose. This is called “sterile technique” and it is also employed in the manufacture of the radiopharmecuticals in the radiopharmacy or the “hot lab” in North American parlance.
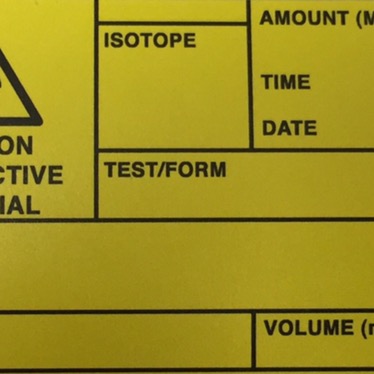
The kit from which the dose was drawn and the amount of activity in the dose is checked. The dose drawn is measured in a dose callibrator that is set for the correct isotope contained in the radiopharmaceutical that is going to be administered. The dose number and activity is entered into the computer in the patient notes section and a hand written tag is attached to the dose which is then shielded and placed into a lead container and transported through the magnetized doors into the injection room. Each one of the aforementioned steps is double checked.
Once the dose is brought into the injection room the patients details are brought up on the computer and the patient is brought into the room. Two people identify the patient by checking the name, first line of their address as well as their birthdate. It is then useful to ask some background info regarding why they are here and then check for contraindications that would prevent continuing on with the procedure.
Only one person injects the dose. The most popular spot to inject a dose is the ante cubital fossa veins. These are the veins found in the bend of the elbow. They are usually prominent on people and are easily accessible for injections. Most injections are done using butterfly needles and some are done using cannulas. Cannulas are a bit more work intensive but the injection has less chance of extravasating and this method is used when there is only one shot at getting the injection right. It’s not a gurantee but the chances are significantly increased.
Once the dose is injected the patient is sent off so that the dose clears the bloodstream and is absorbed into the desired target organ that is to be evaluated. All the details of the injection are then entered into the system and the process is repeated until all the patients are injected. I figure there are on average 20-40 injections performed in a day. The described procedure is generic and there are variations in it depending on the type of procedure that is required.
Injection time is when some small talk happens. It usually stems from the reason why the patient is there to have a bit of radiation injected into them for the purposes of diagnosing or clearing them of a particular ailment or condition. Each person is unique and yet their individual experiences fall into patterns based on what kind of condition they are dealing with. Their personality comes out and as most are elderly they each have a whole lifetime projected through the characteristics of their faces.
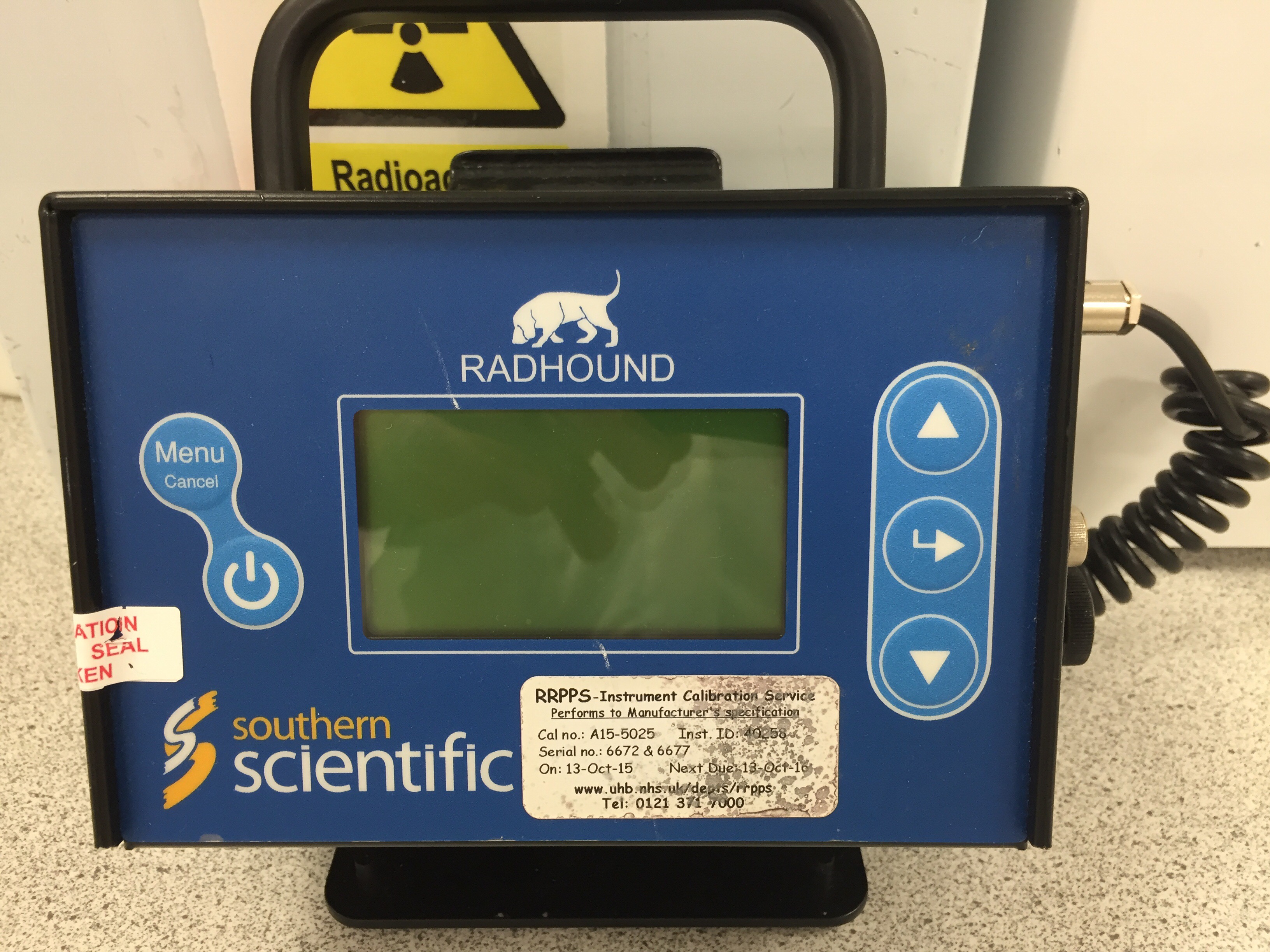
The first time it happened I wasn’t aware when in particular it happened. I suspected something was wrong when I walked by the monitor outside the dispensing room and the counts spiked. I checked my hands and there wasn’t anything on them. Later on when a colleague turned on the monitor to check something the high background was suspicious and as soon as the probe was pointed towards my trousers the counts spiked. We talked about it and made light of the problem and the procedure is to remove the contaminated item. I had to put on a pair of scrubs. The bright baby blue is in stark contrast to the black or navy blue that is required standard uniform attire mandated by the trust. There was no end to the comments by my colleagues for the remainder of the day. It’s all in good fun “I am human after all” and sometimes mistakes happen.
The next day it was a bit different. I knew exactly when it happened. It was close to lunchtime and the day has been busy with a lot of injections. I hadn’t had a coffee break and I was going to sneak one in right after this last injection. The patient was a gregarious lady with whom I was chatting after carefully examining and venipuncturing her vein on her only available arm. “Olde faithful” I remarked as I taped the blur butterfly in place and released the turnoquet. The preliminary flush flowed smoothly and easily into the vein a successful injection. I carefully removed the needle from her dose and then bent the tube and removed the saline. This prevents the backflow of the saline in the line. Attaching the dose to the female end I injected and flushed the dose making sure I got all of her sub milliliter volume of the dose into her. As I removed the dose and replaced the syringe with the saline flush I watched as the needle that has been sitting on top of the trolley roll and bounce off of my one and then onto the floor. I said “fuck” quietly inside my mind and continued on as if nothing happened removing the butterfly and placing the rolled up gauze followed by tape onto the injection site. I reminded the patient of the final instructions regarding when to come back and leading her out of the room.

There are three principles of radiation safety
- Time
- Distance
- Shielding
Minimize the time spent close to the source. Absorbed dose is a function of time and the intensity of the source leading to the second principle that of distance. Think of a candle in your hand. If you hold it close to your eye it is bright and the further away it is the dimmer it becomes. Intensity decreases the further away you are from the source thereby decreasing the amount of exposure you get. Shielding is the prevention of exposure by placing a barrier between yourself and the source.
I picked up the needle from the floor and disposed of it into the appropriate hot sharps container. I found three drops on the ground where the needle impacted the floor. I used a few alcohol swabs to wipe the area in order to absorb some of the fluid and to mark where it is. You wipe towards the centre of the contamination in order to contain it. I then covered it with an absorbent trip as and then placed a piece of lead shielding on top this shields it. With radiation it’s important that the shielding is dense as the energetic power of the radiation passes through lighter materials. Lead is a pretty dense material.

There were three drops where the needle bounced off of my knee. With my head low I sheepishly went to change into scrub bottoms again. My colleagues got a laugh out of it again. The more something gets used the more likely that an accident will happen. There are strategies for dealing with such circumstances and this is all part of the training. Later on the other colleague that I was injecting with had to change as well as she had bodily fluids leak onto her trouser as they were testing an indwelling cannula on an inpatient. Obviously it was faulty and as I went to deal with them to see if I could help I realized the problem. The patient was really poorly with different parts of them swollen with lymphadenopathy. As I spoke to them it became clear that they didn’t want to have any attempts made on accessing their veins. It would have been a difficult task. I’m glad that they made that decision.
Are you going to go for three in a row tomorrow?
That was the challenge cheekily suggested. I don’t contaminate myself often and the past few days were just a reminder to be careful and conscious of what I am doing. The exposure I get is roughly twice what a normal person gets which is low.
